
What is BPPV?
BPPV stands for Benign Paroxysmal Positional Vertigo. It is the most common inner ear disorder and cause of vertigo. Vertigo is as a false sensation of motion. Often described as a spinning sensation or a false sensation of the world moving around you. Vertigo is often intense and can be anxiety provoking to the individual who is experiencing it. Vertigo can also lead to nausea and vomiting. BPPV attacks are provoked by positional changes (i.e. turning in bed, looking up etc.) and are short in duration lasting approx. 1 – 2 minutes. Some people describe a feeling of unsteadiness for a period of time after the attack. BPPV can occur in people of all ages, but is most common in people over the age of 50.
What causes BPPV?
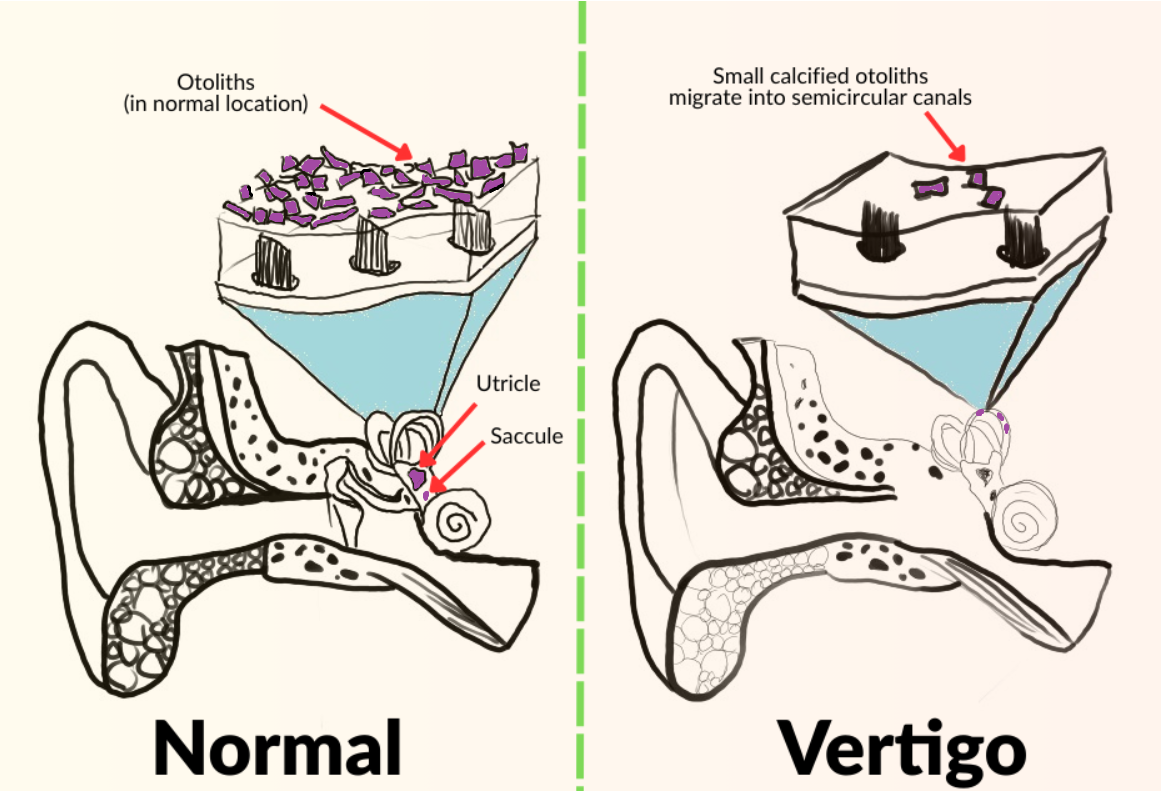
BPPV is the result of otoconia (calcium carbonate crystals) becoming detached from their home in the inner ear and falling into one of the three semicircular canals also within the inner ear. The most common canal these otoconia fall in is the posterior canal due to its position within the inner ear relative to gravity. Otoconia are normally found in the utricle and saccule. The three semicircular canals, utricle and saccule are all parts of the inner ear. The semicircular canals sense head rotation (angular velocity) while the utricle and saccule sense gravity and linear acceleration. For more information about the functioning of our inner ear see the article, “Where Does Our Balance Come From.”
The otoconia dislodged in a semicircular canal makes the canal sensitive to gravity, which is not the canal’s normal function. The otoconia will move the fluid within the canal, which disrupts normal fluid flow. This fluid disruption stimulates the vestibular nerve which sends conflicting information regarding head movement to the brain. This information is conflicting because it does not match information that is being sent to the brain from the other balance systems. This conflicting or false information being sent to our brain leads to vertigo and nystagmus (rapid involuntary eye movements.) Movement of the otoconia within the canal is brought on by changes in head position. Therefore BPPV is position dependent, often brought on when someone is looking up, down, or rolling over to get out of bed.
BPPV can occur without any known cause or event. BPPV can be seen post head trauma, as a result of primary or secondary effects of aging, and can occur secondary to prolonged periods of bed rest. BPPV is also linked to other diseases and / or medical issues such as diabetes, vitamin D deficiency, migraine, Meniere’s Disease, cardiovascular diseases, stroke and inner ear infections.
BPPV Diagnosis
If a medical professional suspects BPPV after obtaining a detailed medical and subjective history regarding a person’s dizziness, they will take their patient through a vertigo provoking maneuver. The maneuver or maneuvers performed will involve changes in head and body positions which will provoke a specific nystagmus pattern. The nystagmus pattern produced will be dependent upon which semicircular canal the otoconia have resided in. The medical professional interprets the nystagmus pattern to either confirm or rule out BPPV. The most common vertigo provoking maneuver is the Dix-Hallpike maneuver which tests for posterior canal BPPV. Posterior canal BPPV is the most common form of BPPV, the others being horizontal (a.k.a lateral) canal BPPV and anterior (a.k.a superior) canal BPPV.
BPPV Treatment
BPPV can be resolved through Canalith Repositioning Maneuvers (CRM,) best provided by a vestibular therapist. Canalith Repositioning Maneuvers involve taking the patient through a series of head positions which allows gravity to help the otoconia move through the canal and return them to where they’re supposed to be. Going through the maneuver will provoke symptoms as the otoconia moves through the canal. Each position in the maneuver must be held for an appropriate period of time (at least 1 min) to allow the otoconia time to get where they need to go.
The maneuver chosen is dependent upon which canal the otoconia resides. The most commonly known maneuver is the Epley Maneuver, which resolves Posterior Canal BPPV. However, the Epley is not the sole maneuver which can be utilized to resolve posterior canal BPPV. A vestibular therapist may utilize another maneuver based upon the patient’s mobility and / or comfort.
A vestibular therapist, which is a medical professional who has been specifically trained in the treatment of vestibular disorders, is best suited to lead a patient through CRM. Most medical professionals will most likely only be familiar with the most common form of BPPV and they may recommend the patient let the condition resolve on its own, or they may inappropriately treat BPPV symptoms through use of medication. There is a chance that BPPV can resolve on its own, however, this is not best practice due to the distressing nature of BPPV, its high correlation to falls and the chance that BPPV can also be confused with other conditions that closely mimic BPPV, such as a brainstem stroke. Therefore, self treatment of BPPV is discouraged. Any neurological conditions that accompany vertigo such as difficulty swallowing, difficulty speaking, fainting, upper extremity or lower extremity weakness, severe headache, or prolonged dizziness will not be solely BPPV or even BPPV at all, therefore a person should seek medical help immediately.
Having issues with vertigo or dizziness? Click the link below to consult with your vestibular and balance specialist.